
LIFE. DEATH. DECISIONS THAT MAKE THEM COUNT.
TO ANSWER this question, let’s make sure we agree on 4 basics.
Then we can figure out how many Australians could die this month [April, 2020].
And when we can dare to live again.
And why we need to.
Because we’re going to be ok, more than ok, a lot sooner than anyone thinks.
‘Cos what if I said the corona virus doesn’t kill you?
It just attacks your body, lets your lungs fill with liquid & makes you NOT breathe.
Not breathing kills you.
Of course, when the air sacs in your lungs fill with water or body fluids, it’s called ‘pneumonia.’
Pneumonia is usually brought on by catching some kind of virus or bacteria.
It is always a horrid experience & often has a ‘glass-like’ effect on the lungs, like this year’s COVID-19-Pneumonia.
And it is already the 4th leading cause of death in the world EACH YEAR. In other words, every single winter the world faces an epidemic of pneumonia.
Why do things look so different this time? After all, as the World Health Organization [WHO] says, ‘this is a controllable pandemic’. And seen in the context of what would normally happen in a COVID-family viral spread [which is what most other colds and flus are], it IS truly amazing and wonderful that we’re doing so well at changing the course of history !
Since we’ve learnt to wash our hands and be respectful of not passing germs to others, we’ve managed to keep community-acquired influenza and pneumonia from reaching the expected annual toll that all trained doctors in each country are always ready for - meaning :
Usually, 3 million at-risk people die from viral & bacterial pneumonia every year.
This year, to date, less than 2% of the normal amount of deaths [approx 60,000 on April 4] & less than 5% of expected pneumonia Hospitalizations have occurred AS A RESULT OF COVID-19 VIRAL INFECTION.
So, is it wise to add a huge additional pandemic of fear about death this year?
And do we need to keep being petrified to leave our homes in case we silently kill or are killed?
Or can we, conversely, congratulate ourselves for our heroism, for compassionately keeping everyone safe now?
Or should we rather be HORRIFIED, or unimaginably SAD, that we’ve been SO incredibly SELFISH and disrespectful till now, as to not notice this huge epidemic of similar deaths [and their consequent burden on all world health systems] in the past ? !!!!
And should we feel guilty for not-knowing ?
Or live in GRIEF for the effects instead?
How do we even dare to ask whether we still dare to live?
I grappled with this complex and traumatic question more than half my life.
Its always helped me to think about things logically to help manage my emotions [therapists can also help with this].
So I’ve done the same thing in trying to figure out how to respond to this crisis we’re facing.
And if you’re feeling overwhelmed by emotion in this new situation, I hope my notes below help you or someone you know feel calmer, safer and freer to move again.
Please note that I’m not asking you to believe anything. You should always, always check the underlying facts [and potential financial, political or fame-based motivation as well as qualifications of the speaker] behind every story, to prove things to yourself. I’ve tried my best to link to the sources you need to look at, to examine the evidence and come to your own conclusion that fear is not necessary and does not help us make the right decisions on what to do next.
You can skip to the end of this page, if you’re sure of the basics of how covid-family viruses, bacteria and all kinds of other germs spread, create pneumonia, affect hospital loads & potentially kill patients every year. But please do read to the end of my whole essay before you object to, or agree with, the actual point I’m trying to make.
And if you’d like to comment on, or correct errors in, my hypothesis by giving better, real data, please come out of hiding & talk with me !.
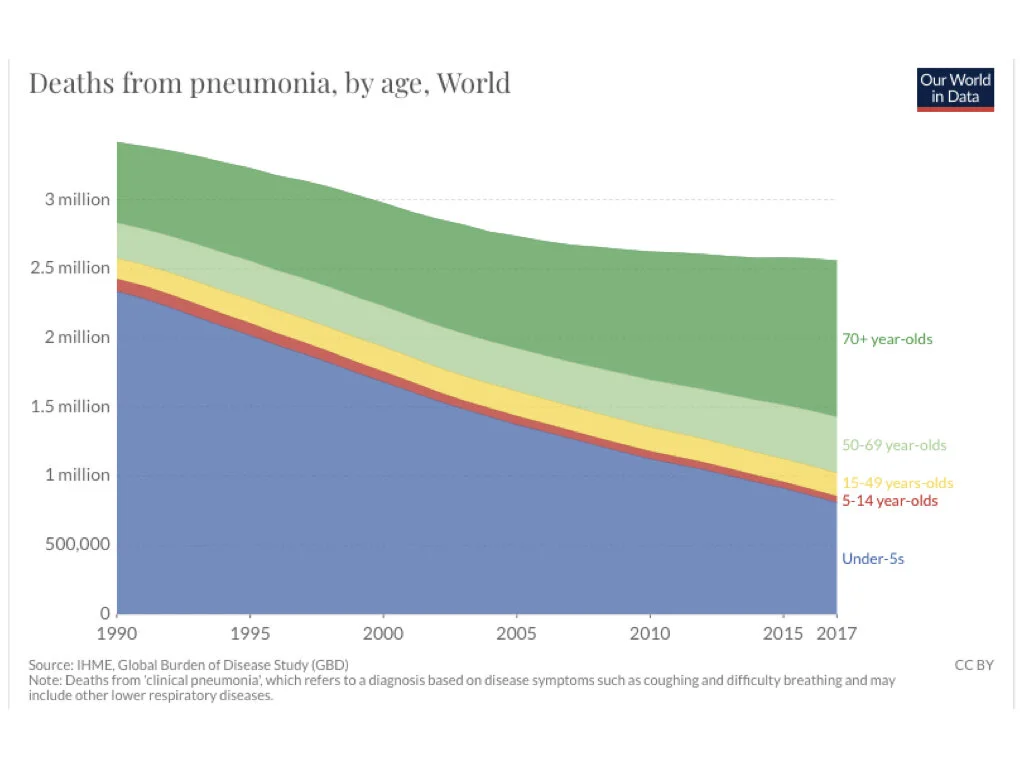
Deaths EACH YEAR from COVID-related influenza induced viruses and bacterial pneumonias. From Our World in Data https://ourworldindata.org/pneumonia
1. WE WANT TO HELP ALL HUMANITY, SO WE’RE WILLING TO BE IN QUARANTINE RIGHT NOW.
We’re told that not all countries have enough spare beds to accept an additional influx of patients with a new, unknown virus. Many have only enough hospital beds and critical care units to cope with the number of cases they already expect from known diseases & accidents. So, if a hospital with only 10 critical care units is already 80% full, and suddenly gets 10 new patients who need those beds and ventilators, it can only accept 2 of them - it has no room or equipment to help 8 of the new patients.
Apparently, the COVID-19 virus spreads approximately twice as fast, or to twice as many people in a given timeframe, as other COVID-family flu viruses.
Social distancing and keeping clean helps slow the spread of ANY virus, so that even if the same 10 people are still eventually, karmically destined to get a given disease and inevitably need medical help, they will not all get sick and need help at once!
That means hospitals will be better able to cope. They will not be faced with too many unexpected patients in one week, but can instead accommodate them over one month. On a mathematical graph, the time difference between the two scenarios shows up as the difference between a big hump in the first case without social distancing to curb infection rates, and a long, low, ‘proverbially flattened’ curve if we slow the spread.
2. WE’re preventing death by ‘FLATTENINg The curve’ - OR ARE WE? France and Germany TODAY.
They are respectively 4th and 5th worst, on the list of most infected countries.
Germany, with 60,000 reported cases, has a mortality rate of only 0.9%. Yet France has approximately 35,000 cases today, and a mortality rate of 6.8%.
In the worst imaginable historical disaster [eg. The Bubonic Plague], 50% of patients infected by a new unknown disease are hit badly enough to need hospitalisation they can’t get and 10% of the infected require critical care [or ventilators in today’s terms].
Thankfully, right now, the truth seems to be that fewer than 20% of COVID-19 infected patients require hospitalization and less than 5% require critical care. So France and Germany today might need, respectively, 1750 and 3000 ventilators each.
That’s an awful lot more ventilators needed in Germany than France.
And yet they already managed to stop the epidemic escalating in their country !
Why is this? Because they were prepared? Because they know that, in any ordinary year, run-of-the-mill [COVID-related] influenza-induced plus bacterial pneumonia is already the 4th leading cause of death in the world - up to 3 million deaths annually across all age groups - 230,000 of these in Europe. Because they know that this class of disease has a critical care and mortality rate of between 4% and 9% ? And because they know that Germany, in particular, has the second highest number of deaths from all pneumonia in Europe each year, averaging 16,000 ?
Or do they simply accept that our body is impermanent and death is an inevitable consequence of life?
Maybe.
It turns out Germans already have 25,000 machines available [more than double what they need for these kinds of deaths every year] and can easily make more.
Whereas apparently France seems to have never had enough existing ventilators to cope with demand in its hospitals in previous years, nor does it have French companies who make them. That sounds strange and sad, doesn’t it? But maybe the French know that ventilators can also INCREASE the risk of dying from pneumonia?
3. WHY WE CAN’T BE SURE ABOUT cause & EFFECT - the FIGURES WE HEAR IN THE MEDIA.
The amount of testing we do changes how we see any disease progress and how we count the % of deaths.
% of Deaths [mortality] is calculated as : How many die /How many confirmed positive cases of a disease x 100.
Or, more strictly speaking: How many die /How many people are either scared or sick enough to go to hospital and are confirmed positive x 100.
The thing is, a million people or even the entire population of France - or the world- could be infected by now. We don’t really know how many have the virus, because [i] we don’t test everyone and [ii] carriers don’t show symptoms! And if we insisted on testing everyone who isn’t going to the doctor because they have only mild flu-like or no symptoms [who of course will still test positive], then the total cases [the bottom or right side of the equation] would be huge !
As a result, the % number of Deaths per total infections [final figure after calculation] would look lots smaller!
Indeed, as more data comes in, and the world seems to cope better with the progression of the novel disease, health professionals are starting to suspect we actually have a world average of 2 - 3.4 % mortality.
This is a lot lower than the normal mortality rate [of 4 to 9%] from all other types of pneumonia, that I pointed out earlier!
Here’s a SUMMARY OF MORTALITY RATES FOR SELECTED COUNTRIES
deaths / confirmed infections x 100 on MARCH 31st, 2020
calculated from WHO CoVid-19 Report 71, Table 1
Over 100,000 Total Cases
United States 1.7%
Italy 11%
Over 75,000 Total Cases
China 4%
Spain 8.6%
Over 50,000 Total Cases
Germany 0.9% - AMONG THE LOWEST IN THE WORLD
Over 35,000 Total Cases
France 6.8%
Over 20,000 Total Cases
UK 6.3%
Less than 10,000 Total Cases
Korea 1.6%
3000- 5000 Total Cases
Australia 0.41% - AMONG THE LOWEST IN THE WORLD
Singapore 0.34% - AMONG THE LOWEST IN THE WORLD
Israel 0.35% - AMONG THE LOWEST IN THE WORLD
Norway 0.6% - AMONG THE LOWEST IN THE WORLD
Sweden 3.6% - NOT HIGH CONSIDERING THEY’RE NOT DOING SOCIAL ISOLATION AS THEY ALREADY SPEND TOO MUCH TIME ALONE
Brazil 3%
Denmark 7%
Less than 2000 Total Cases
Iceland 0.18% - THE SECOND LOWEST IN THE WORLD
Estonia 0.4%
Kazakhstan 0.3%
Diamond Princess Cruise 0.98%
Slovakia 0% - THE LOWEST IN THE WORLD
AND
Thailand 0.6%
Japan 2.8%
India 2.7%
Indonesia 8.6%
AND
Chile 0.32%
Peru 1.2%
Colombia 1.4%
Mexico 2%
Argentina 2.4%
Ecuador 6.4%
SO now let’s look at WHAT THIS MEANS FOR australia IN PARTICULAR
Yesterday [March 31st] in Australia, we recorded our 21st death from the disease. Total.
So at our current mortality rate, we could extrapolate that 100,000 might die from this, if every single person in the entire country were infected. In that case, with the split of infection between states you can see in the Table from the Australian Government Department of Health below, we’d see up to 50,000 people die in Sydney alone and 20,000 in Victoria.
That seems to be what everyone thinks will happen.
![Table from Australian Government Department of Health on March 31st, 2020. Coronarvirus [COVID-19] Current Situation & Case Numbers](https://images.squarespace-cdn.com/content/v1/55c77a9ae4b0760916a638b9/1585980459467-36G6L0LZATTVB2QIIXD9/AusGov_March31.001.jpeg)
Table from Australian Government Department of Health on March 31st, 2020. Coronarvirus [COVID-19] Current Situation & Case Numbers
BUT there is AT LEAST one important piece of information we seem to have forgotten.
If you remember Tomas Pueyo's article in Medium - his Chart 7 in particular - Wuhan closed their city when they reached 400 confirmed infections per day. From that day, their reported infection curve started to fall.
And two days ago on March 30, Australian TV news told us that Wuhan reopened. In other words, it took them 2 months from the official lockdown to open their doors again.
Also, we know that China's total case count [including those who died] is currently around 75,000.
Remember infections are the cases. Cases do NOT equal hospitalizations!
Australia closed its borders a long time before it recorded 400 CASES per day.
That means, on the curve from Tomas’ graph, we started isolation a lot earlier and will see results much earlier than Wuhan.
That’s not to mention the fact that, as a country, our living conditions are such that we're more isolated from each of our fellow 22 million Aussies over our millions of square kilometre country than the Wuhanese are from each other, with 11 million people packed into an urban 8,500 km2.
We simply cannot infect each other the same way.
THAT MEANS OUR CURVE WILL, DEFINITELY, BE MUCH FLATTER THAN THEIRS.
The total number of infections we can expect almost definitely can’t exceed Wuhan or China's 75,000.
THOUGH let’s imagine that, for some completely off-the-charts karmic reason,
we did actually reach that same number of confirmed infections.
Even then, at our current Australian mortality rate, the number of deaths we can expect from coronavirus in the country as a whole, also won’t exceed China’s.
WHAT if we use the final total infections in China as our worst scenario & project what the Australian situation WOULD be THEN ?
THE WORST CASE SCENARIO WE CAN HAVE IN AUSTRALIA IS ONLY 15X BIGGER THAN TODAY.
and if we add up all 11 things we KNOW about the virus:
Infections become obvious within 4-14 days of exposure to the virus.
At least 25% of people will show no symptoms whatsoever, according to both Chinese scientists and the US Center for Disease Control and Prevention.
Perhaps another 50% have mild enough symptoms that they require no hospitalization and which may or may not be tested and officially recorded.
A rounded maximum 25% of infected patients may therefore require hospitalization - these are definitely ‘recorded cases’ we measure in our statistics and hear about on TV.
Of infected patients, perhaps 5% may be so critical as to require ventilators.
99.1% of deaths occur in patients with up to FOUR serious pre-existing health conditions such as diabetes, asthma or other lung conditions, high blood pressure and heart disease. These are the same kinds of people who would, in any other year, also be most at risk to be hospitalized and potentially die from pneumonia complications after catching a known, COVID family virus-induced influenza, or bacterial influenza or both.
The median age of death in Italy is 82. The CDC in the USA also reports older Americans represent 80% of deaths. However, mortality figures in all countries vary for different ages depending on the demographic of the country. So countries with a younger average population overall will have a lower average age of mortality.
UK Government scientific advisors have calculated the overall chance of any one person dying from the disease is 0.5 - 1%. This is lower than the rate of death among confirmed cases because not all infections are confirmed by testing.
In anyone with few or no symptoms and healthy immune systems to remove the offender, the virus will be gone from the body in a few days or at most a few weeks [and gone from all touched surfaces within 5 days, with the risk reducing by half, every hour]. As far as scientists know, on a par with other corona-based colds and flus, no one will remain a carrier for months or years [ie. it’s not like malaria, for instance].
In the context of up to 3 million deaths normally recorded each winter from COVID family and bacterial pneumonia worldwide, the current tally of 60,000 deaths from the COVID-19 strain is 2% of what we would normally prepare for.
The Australian mortality rate [calculated from WHO data on March 31] is 0.41% of reported infections.
and if we believe these statistics are true and treat them as a whole, the way we would consider ALL EVIDENCE in any other scientific situation where we weren’t afraId of dying, then WE would ALSO now KNOW THAT AUSTRALIA’S EXPECTED DEATHS FROM COVID-19 SHOULD BE NO MORE THAN 308 PEOPLE IN TOTAL OVER ALL THE SHORT [!] TIME THE EPiDEMIC LASTS.
Yes, we need 18,750 hospital beds for patients with this particular viral pneumonia countrywide - with 50% of these in Sydney [9,375] and 20% [3,750] in Victoria. But don’t forget to compare this with the normal 77,000 hospitalizations we know to expect from all viral and bacterial pneumonia in the at-risk group in Australia each year.
Yes, we may need 3,750 ventilators in total [of which 1,875 in Sydney and 750 in Victoria] in the next two months.
And yes, 308 people will presumably die from the novel COVID-19 strain in all of Australia - half in NSW and [20%] 72 of them in Victoria in the next two months - and please try to consider this, in light of knowing three years ago, in 2017, a total of 4269 patients died from pneumonia in our country [that was an average year].
but we should not need to expect more. Because anyone who does not show symptoms of the virus by the 14th day after the lockdown which officially started in Victoria on March 28, can be assumed to be free from it.
And, assuming we haven’t allowed new people into the country without quarantine, and assuming we keep the [by then] known, actually infected persons and families - and their caretakers and families [if cohabiting] - separate from everyone else, it will take us a lot less than the 2 months it took Wuhan to clean up, since we started the process much earlier.
Likewise, any country or state that closed its borders before the 400 daily case mark was reached, and which has a low mortality rate [eg. 2% or half the normal minimum annual rate of death from pneumonia each winter] could be expected to have enough hospital beds to cope with the situation and will hopefully be in the same category we are [Hello Mexico].
Now, of course these are not final, definitive statistics. There are a huge number of unknowns yet to be known, and I am in no way suggesting I know them now - I’m just a simple scientist and meditator, trying to figure out the truth!
And of course we shouldn’t, willy nilly, extrapolate these figures to New York or London, where infections have happened faster, so quickly add up to be greater and therefore make mortality totals much higher.
Though at the same time, we should remember that New York is America’s Wuhan. As many have pointed out, the scary story going on there is not representative of what’s going on in the rest of America - California, for instance, isolated its population from each other and incoming visitors a long time before reaching the 400 daily case mark too.
We’re going to be ok soon, a lot sooner than anyone thinks.
AS LONG AS WE LOOK AT THE SCIENCE, NOT JUST THE NEWS.
Basically, what I’m trying to say is that, as far as I can figure out, in Australia today, there is no reason on earth why we need to prepare for hundreds of thousands of hospitalizations and tens of thousands of deaths.
Nor should we make the mistake of believing dramatic, out-of-context reports of individual or celebrity patients in the media represent the totality - or even approximate reality - of our situation, rather than suspect myths or mere sensationalism of billionaire-owned, broadcast news.
Of course, I’m not advocating we should throw caution to the winds and run out and party in the streets as soon as our first 14-day quarantine period is up.
I’m not suggesting we should re-open the borders at Easter and welcome visitors from seriously infected countries.
And God forbid we should stop washing our hands or looking after each other. That’s a given, even without viruses.
But at the same time, we should think about the implications of the 11 points listed above, seriously too!
those 11 things we know about the virus tell us Australia does NOT need to keep everyone in quarantine for months on end. We CAN probably be safe WELL bEFORE the end of April.
Definitely, we do not need to stop our world for a year with military insistence.
4. So NOW WE CAN ASK, how do we dare live when loved ones are dying?
Each year in Australia, approx. 106,950 people also die from cancer, also usually requiring critical care in their last weeks.
That’s around 300 people per day, a light-year worse than the 7 deaths reported from COVID-19 in all of Australia on the day of April 3rd., 2020.
Their deaths don’t stop the economy.
Especially if they are our loved ones.
Rather they do the opposite.
Just like a real war does.
Just like my father did for me.
In his 18-year battle with cancer and associated complications [following all the other 17 years of life-threatening illnesses and accidents he’d had prior], he never once, in all that time, made my family feel guilty for living, while he was suffering.
You see, the immanent sickness, death and loss of our loved ones is supposed to inspire us to do something good with our lives and not sit on our backsides watching Netflix in a cave, accepting masked, armed forces telling us we must sit in the dark till we die. We’re supposed to come to the conclusion Buddha came to, when shocked into his first experience of this truth.
Because one day, for sure, every single one of us will die.
So we must make the most of the precious opportunity we have, to live our highest purpose, help others & love as much as we can.
if we use this situation wisely, we will not let this virus or anyone else trick us into thinking our biggest challenge is about avoiding physical death. We’ll be able to learn from feeling the pain of the truth of our mortality, not seek to avoid it.
And then, if we’re lucky, this time in history can be one of the biggest opportunities we will get in our lives, to rethink how we’ve been living and what we’ve been doing, so that this kind of thing never happens again.
We can choose to let go of those ambitions & attitudes, jobs & companies, environmental impacts, political & health concerns that the virus has shown us are nowhere near as important as we previously thought they were.
And possibly, maybe, we can collectively figure out how to meet the mental and spiritual crisis that underlies the physical one - how to unbreak the world as soon as possible and restore, remake and reinvent our future with grace, gratitude and awe.
If you want to comment - or correct any errors in my hypothesis with real data, please come out of hiding & talk with me !